


Overview
Scleroderma is an autoimmune disease (autoimmune = immune system targets the patient’s own tissues) characterized by an excess formation of fibrous tissue (scar tissue) in various organs including the skin, lungs, heart, intestines, that cause these organs to not work properly.
faqs
How common is scleroderma?
Scleroderma is a relatively rare disease affecting about 2.5 of every 10,000 people. By contrast, rheumatoid arthritis affects about 50-100 out of every 10,000 people. Scleroderma occurs more often in women and in African-Americans.
What causes scleroderma?
Like most autoimmune diseases, an interaction between a person’s genes and the environment leads to the development of illness. There are multiple genes implicated in scleroderma and the end result is the development of immune cells, antibodies, and cytokines (inflammatory chemical messengers) that promoted the development of a pro-fibrotic process in the body. TGF-b or (transforming growth factor beta) and IL-6 (interleukin 6) are important cytokines that stimulate fibroblasts to produce more collagen that causes the tissues and blood vessels to thicken.
What are early symptoms of scleroderma?

young woman showing blanching phase
The majority of people with scleroderma will first have Raynaud’s phenomenon which causes the hands and feet to blanch with cold exposure. It is important to remember that many people have Raynaud’s phenomenon but most will never develop scleroderma. The people with benign Raynaud’s phenomenon generally develop the condition during teen years or as a young adult. The people of most concern are those who develop Raynaud’s phenomenon later in life and progress on to develop skin changes. Sometime after the Raynaud’s starts, the hands may become puffy and swollen and the fingers become difficult to bend. In milder cases, the fingers may become slowly tight over months to years.
Are there different forms of scleroderma?
There are three basic types of scleroderma:
1. Diffuse scleroderma - this is the most severe form of disease with the most extensive thickening of the skin and internal organs. Symptoms can begin rather rapidly.
2. Limited scleroderma – skin and organs are in general in less intensely involved. Changes may not be unrecognized for month to years. Internal organ changes are generally less severe but lung disease can occur.
3. Scleroderma sine scleroderma – internal organ fibrosis occurs without skin involvement. This is the least common form of scleroderma
There are 2 localized forms of skin disease that do not have any organ involvement. One is called liner scleroderma and the other is called morphea.
What blood tests are helpful?
There are several antibody tests that may help characterize the disease. The table lists some of these antibody tests and their meaning.
|
Antibody test name |
Abbreviation |
Association(s) |
|---|---|---|
|
Positive antinuclear antibody test with nucleolar pattern |
ANA nucleolar pattern |
Seen in people with lupus or diffuse scleroderma |
|
Positive antinuclear antibody test with centromere pattern |
ANA centromere pattern |
Seen in people with limited scleroderma |
|
Scleroderma 70 antibody aka topoisomerase 1 |
SCL 70 |
Seen in approximately 50% of people with diffuse scleroderma and increases the risk of lung disease |
|
Centromere B |
Same |
Confirms centromere pattern on ANA and seen in those with limited disease |
|
RNA polymerase III |
RNA Pol III |
Seen in people with diffuse disease and associated with more severe skin hardening and also with kidney disease |
What are the manifestations at each organ?
Skin – the skin can be thickened and makes moving of joints difficult. It can happen rapidly in patients with diffuse disease and these patients can also develop puffy hands. Patients with limited disease may slowly note difficulty making a fist and thickening of the fingers. The skin over the hands, face, trunk, arms and legs, and feet can also be affected depending on the type of scleroderma. As the disease progresses, ulcers can develop over the skin especially over the knuckles and be very hard to heal. Some people also develop calcinosis or calcium deposition in the skin that can be painful.
Joints – up to 10-50% of people with scleroderma will develop joint inflammation mostly hands and wrists. Up to 5% of patients will develop an overlap with rheumatoid arthritis including the same blood tests one sees in classic rheumatoid arthritis (rheumatoid factor, cyclic citrullinated peptide.

Muscles – 10-15% of patients will develop muscle inflammation that can cause muscle weakness especially in the shoulders and hips. Patients with muscle involvement have a hard time lifting their arms over their head and getting out of a chair.

calcium deposition in the tissues.
Blood vessels – Raynaud’s phenomenon is almost universal in people with scleroderma affecting over 95%. It can be as mild as numbness and tingling with color change. The condition has three color changes. First white when the blood vessels clamp down (noted in picture above), blue when decreased blood flow becomes more severe, and finally red when the blood vessel open up and blood flows back in the fingers or toes. Most people just have the white phase but in some people the Raynaud’s can be more severe leading to damage of finger tips or skin ulcers requiring more aggressive therapy to try to keep the blood vessels from clamping down.
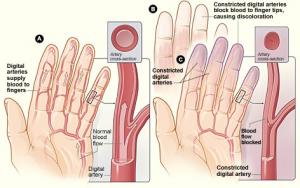
constriction that happens in Raynaud's phenomenon.
Another blood vessel manifestation of scleroderma is pulmonary artery hypertension. This is caused by increased pressure in the blood vessels from the right side of the heart to the lungs. With higher pressure, the right side of heart can begin to fail as it is not use to high pressures that are typical of the left side of the heart that supplies blood to the body. Symptoms of pulmonary hypertension initially is shortness of breath especially with climbing stairs or walking up hills.
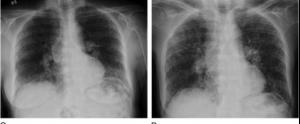
Lungs – Fibrosis can occur the lungs especially at the bases or lower areas of the lung. This is known as interstitial lung disease and comes in two forms; UIP or usual interstitial pneumonitis and NSIP or non-specific interstitial pneumonitis. UIP is more serious and is harder to treat and results in more scar tissue formation while NISP is a bit easier to treat and has more inflammation and less scar tissue formation. Fifty percent of people with diffuse disease and 35% with limited disease will develop lung disease. In some people with lung involvement the symptoms begin quickly but in most it is slow and progressive. Symptoms are progressive shortness of breath that may require oxygen and rarely lung transplantation. Lung involvement can be detected early by a high-resolution CT scan of the lungs and breathing tests called pulmonary function tests.
Esophagus, Stomach, and intestines – Eighty percent of people with scleroderma will have some degree of heart burn where acid in the stomach backs up into the esophagus. This can cause pain and may accelerate lung damage. Also, food may not go down easily due to effects on the muscles of the esophagus. Food will get stuck on the way down and need several swallows or additional liquid to get into the stomach.
The fibrosing nature of the disease can lead to changes in the muscles that help in the movement of food not only through the esophagus but also the stomach and intestines. Feeling full after a small amount of food or feeling constipated is not uncommon. Overtime, the decreased mobility of the intestines can lead to bacterial overgrowth also known as SIBO (small intestine bacterial overgrowth). When this happens people can get explosive diarrhea after a meal and can lead to weight loss. Use of intermittent antibiotic may help this problem.
Some people can develop enlarged superficial blood vessels in the stomach that give the appearance of a watermelon skin. This is called watermelon stomach or the medical name is GAVE or gastric antral vascular ectasia. These vessels can bleed and lead to anemia.
Kidney – Kidney disease is manifested by what is called renal hypertensive crisis that occurs in about 5% of people with scleroderma. For reasons that are unclear in some people with scleroderma a chemical angiotensin which normally helps maintain blood flow to the kidney is markedly elevated and blood pressure is made dangerously high. People with hypertensive crisis can have protein the urine and anemia. Treatment is with an angiotensin converting enzyme inhibitor medication. Some will have permanent kidney damage following an episode and others might need temporary kidney dialysis to allow the kidneys to heal. Risk factors for renal hypertensive crisis include diffuse disease, recent use of high dose prednisone, and the antibody RNA polymerase III. People with limited disease can also develop hypertensive crisis but not as often.
How certain manifestations of scleroderma treated?

Raynaud’s phenomenon – keeping warm is important especially the hands, feet and he body core. A good pair of gloves is important and a pair that includes wind block capability is particularly helpful in Winter. Wearing wool or wool blend socks in cold weather can help keep feet that are often wet, warm in spite of the moisture. The use of wrist wallets with a small hand warmer in the pocket and palm side of the wrist will warm the blood going to the hand.
There are medication that can be used as well called calcium channel blocker that dilate vessels. Nitroglycerin ointment also has some utility in more severe cases of Raynaud’s. Sildenafil is a pill also used in more severe disease.
Gastrointestinal reflux disease – aka heartburn. It is important to not eat late in the evening and also avoid certain food that might cause heartburn such as chocolate or spicy foods. Elevating the head of the bed or sleeping on a wedge can also prevent night time reflux of acid into the esophagus.
There are medication such as the proton pump inhibitors, such as omeprazole, that are very useful and may need to be taken in higher dose and multiple time during the day. H2 blocker such as ranitidine can also be used in milder cases as can oral antacids.
In the most severe cases not responding to local measures and medications, a surgical procedure called a Nissan fundoplication can be done to wrap the stomach around the lower portion of esophagus to help prevent the reflux of acid.
Lung disease – Medications to treat lung disease are generally immunosuppressants. Mycophenolate is one of the principle medications used and has been shown in clinical studies to reduce the progression of the lung disease. Recently, a medication called nintedanib has been approved for therapy of scleroderma lung disease to reduce the progression of fibrosis. It is a newer class of medication called antifibrotic agents. Other medications have been used such as cyclophosphamide, a very potent medication given by vein monthly for 6-12 months. Rituximab has also been used and is given by vein every 6 months. Repeat breathing tests, 6-minute walking tests for distance and oxygen level in the blood, and lung CT scans are used to determine efficacy of therapy. The University of Washington has a clinic focused on the lung disease of people with scleroderma called the ILD/Rheumatology combined clinic. Lung specialists and rheumatologists work together to treat people with scleroderma and lung fibrosis.
Therapy for severe scleroderma
For patients with potentially life-threatening scleroderma the SCOT trial demonstrated the potential benefit of bone marrow transplant to modify the course of disease. The trial compared intravenous cyclophosphamide to autologous bone marrow transplantation (using the patient’s own bone marrow). Bone marrow transplantation demonstrated a survival benefit over the cyclophosphamide. Because of the intensity and life-threatening nature of this this therapy, it is only for the most worrisome patients. The University of Washington was a key participant in this study and Dr. Mark Wener was the University of Washington lead in this important trial.
Getting involved
Supporting Research in the Division of Rheumatology
Those interested in supporting the Division of Rheumatology and its mission to find a cure for autoimmune disease can do so by visiting our Philanthropy & Giving page.